 Two weeks ago I wrote Medical Malpractice – A Primer, directed toward members of the medical community due to a recurring theme I saw on medical blogs: The idea that such suits are brought cavalierly. (You can this in the comments section of blogs such as Flea, GruntDoc, and Kevin, M.D.)
Two weeks ago I wrote Medical Malpractice – A Primer, directed toward members of the medical community due to a recurring theme I saw on medical blogs: The idea that such suits are brought cavalierly. (You can this in the comments section of blogs such as Flea, GruntDoc, and Kevin, M.D.)
I promised a follow-up on how cases are selected by a plaintiff’s attorney, but first want to deconstruct the time and money needed if the matter is taken. For only by understanding the time and money risks can one appreciate the importance of careful screening for potential litigation.
Though all cases are different, let’s assume this simple fact pattern: A 10 month delay in diagnosing and treating breast cancer in a 50 year old woman with a husband and two kids, one of whom is a minor. Her cancer has now spread to two lymph nodes. She has a part time business. All parties and witnesses are local.
The following time and money costs must be assumed to take such a case to verdict:
- Obtain all medical records of any kind for her;
- Expert review on the issue of negligence (perhaps a radiologist or OBGYN, depending on the facts of why the cancer was allegedly missed) prior to taking the matter, intermittent reviews as needed during litigation, and a day in court for trial;
- Expert review on the issue of causation and damages (likely an oncologist), and a day in court for trial;
- Expert review on the issue of lost wages or household services (economist or vocational economist) and a day in court for trial;
- Cost of depositions (doctors, nurses and other witnesses);
- Possible videotaping of depositions for those who may not be present for trial;
- Daily copy of transcripts from trial;
- The purchase or creation of demonstrative evidence to explain the medicine, facts of the incident or injuries to the jury. This could be anything from enlargements of documents and x-rays, to medical models, custom illustrations or video footage, as warranted; and
- Due to personal circumstances of the sick woman and her family, they can’t pay the out-of-pocket costs.
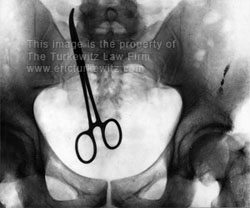
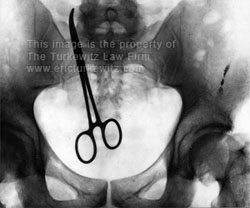
Since the case will always be thrown out without an expert (with the exception of the rare res ipsa case, such as the retained clamp above), the liability and causation experts are not optional.
The attorney’s time involved for litigating the case for a few years will entail record reviews, expert discussions, document drafting, depositions (and prep), possible motion practice, and 5-10 court conferences. It will probably be a two week trial if all goes very smoothly — but depends on the judge’s schedule, the schedules of the experts on both sides, and the longwindedness of the attorneys — and can very easily go longer. It will, in sum, likely be several hundred hours, though it could be more. The opposing attorneys will be top-notch medical malpractice litigators because the insurance companies don’t hire a jack-of-all-trades for this sort of thing.
The out of pocket costs will easily be $30,000 — $50,000, and quite possibly higher depending on the particulars of the case.
If the case is lost at trial — perhaps because of a defense expert who “goes the extra yard” for a fellow physician, a plaintiff less attractive than the defendant doctor, “bad facts” you didn’t know about at intake, a tendency for juries to favor doctors, an unexpected scheduling problem that prevents a witness from appearing, or a plain old dispute as to the standard of care — your money and time should all be assumed to be gone. It is unlikely you will recoup the disbursements from the client. You still have to pay the rent, personnel, utilities, computers and other costs of running a business.
One should never assume that the case will settle, of course, but if it does it will probably only be after you have prepared for, or even started, the actual trial. (See: No, your medical malpractice case will NOT settle fast.)
If you win and get paid back your disbursements and receive a fee, it will still likely take a few years. (You may want it to go quicker, but defendants do not, and the court may not be able to.)
From a cash flow standpoint, this is not an attractive business model. And in New York, those fees if you are successful start at 30% and slide down to 10% as the recovery increases. And if another attorney did some work on the file and then forwarded it on to you, you will be sharing that fee with others.
This, of course, assumes no appeals. If the trial court or appellate thinks the verdict is too high, it will be thrown out. (see, How New York Caps Personal Injury Damages)
In short, the economics from a business standpoint are quite poor, which is why case selection becomes so important for the careful practitioner. It is also why the average malpractice recovery is so high, since the medical community enjoys de facto immunity for smaller cases based on these economics.
To call this a high-risk endeavor would be a significant understatement. The vetting process for such a case is therefore critical, and will be the subject of a future blog posting. [This link added 5/22/07]